Page 10 / April 07
ANSWER:
The patient was prepared for bronchoscopy and gastroscopy under general anesthesia. The surgeon was consulted. We discussed with the parents about the high probability to perform the lobectomy after bronchoscopy and gastrostomy to prevent further aspiration and lung destruction.
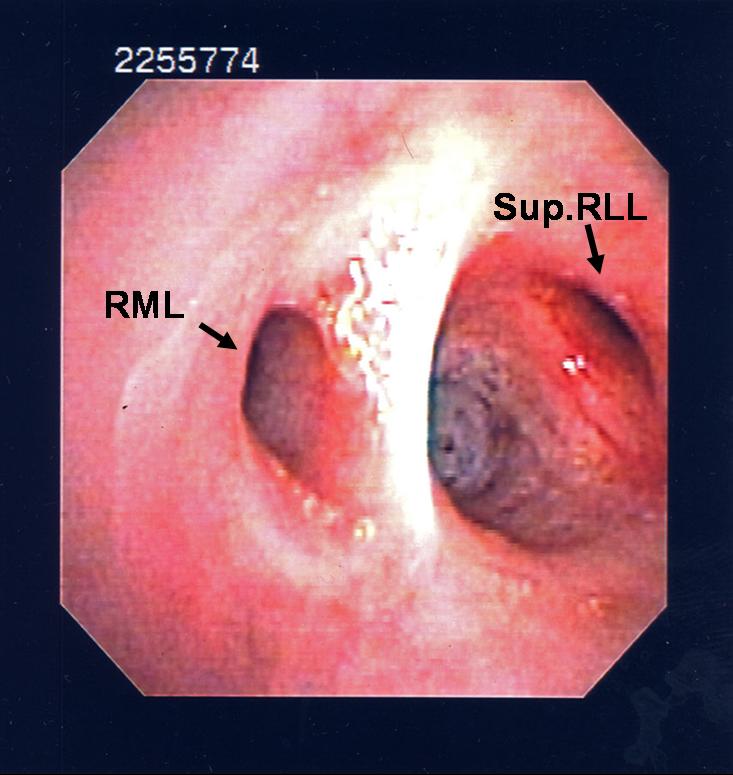
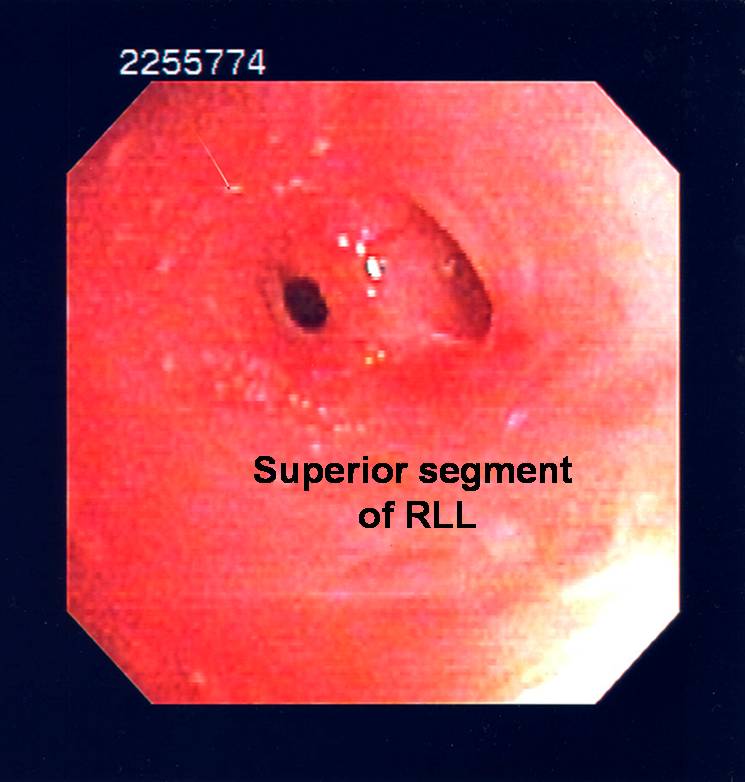
- Bronchoscopy revealed a small abnormal fistula in the bronchus of the superior segment of right lower lobe with whitish mucus plugging. There was no active bleeding nor was an endobronchial lesion found. The bronchoalveolar lavage was done at the superior segment of right lower lobe and sent for bacteriology and fungal culture.
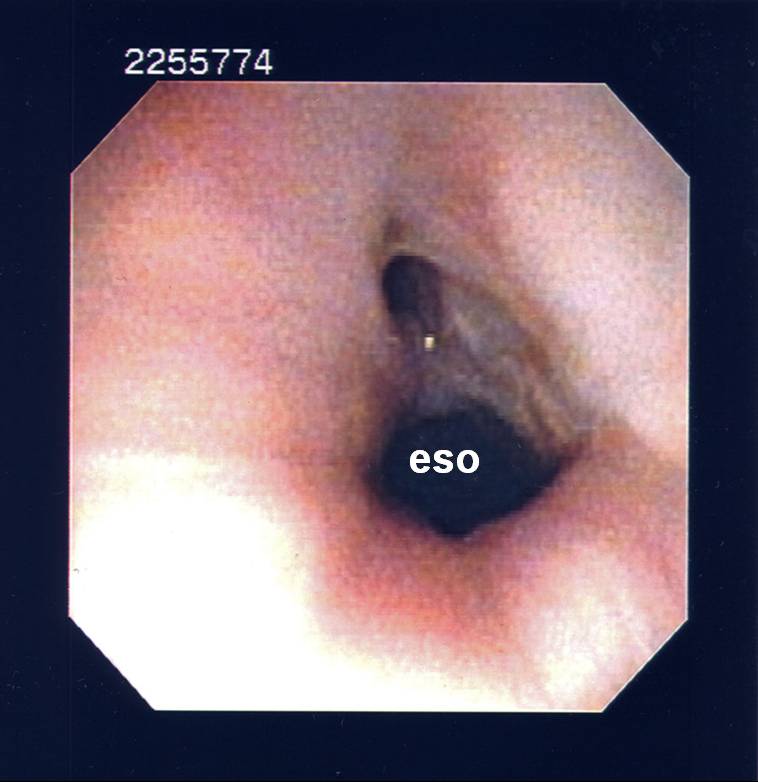
- Gastroscopy revealed a large abnormal connection at the distal esophagus. There was no esophagitis, gastritis or peptic ulcer found.
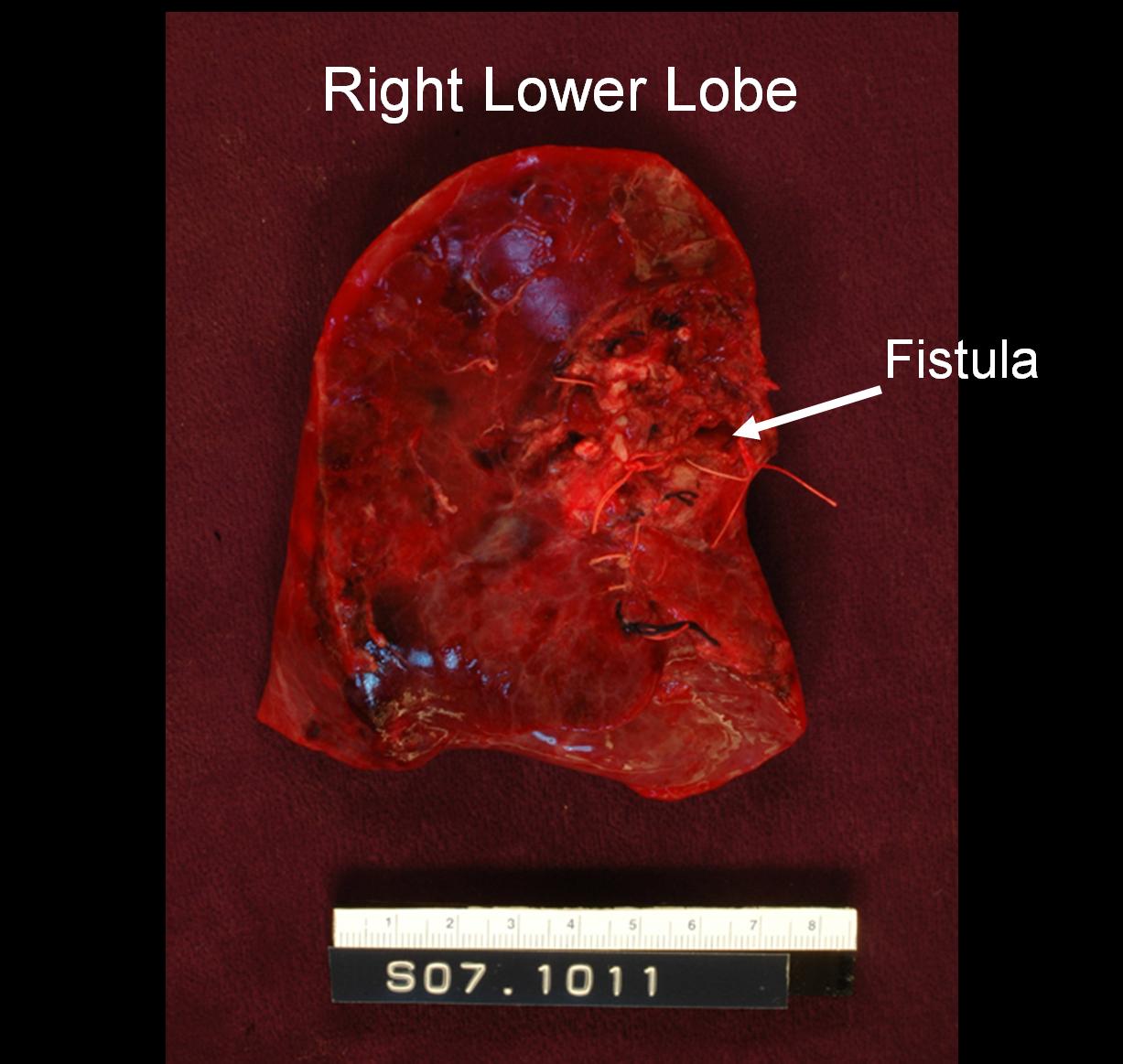
- After these procedures, a right lower lobe lobectomy, fistulectomy and esophageal repair with pleural flap were performed without any complication. The lung tissue was sent for pathology and bacteriology.
The following screen shows the images from the bronchoscopy
|
|
|
| Figure 5-a |
Figure 5-b |
Figure 6 |
Pathology results:
- Bronchiectatic change at right lower lobe area, especially superior segment bronchi with thickened irregular islands of cartilage. (Figures 7-a and 7-b)
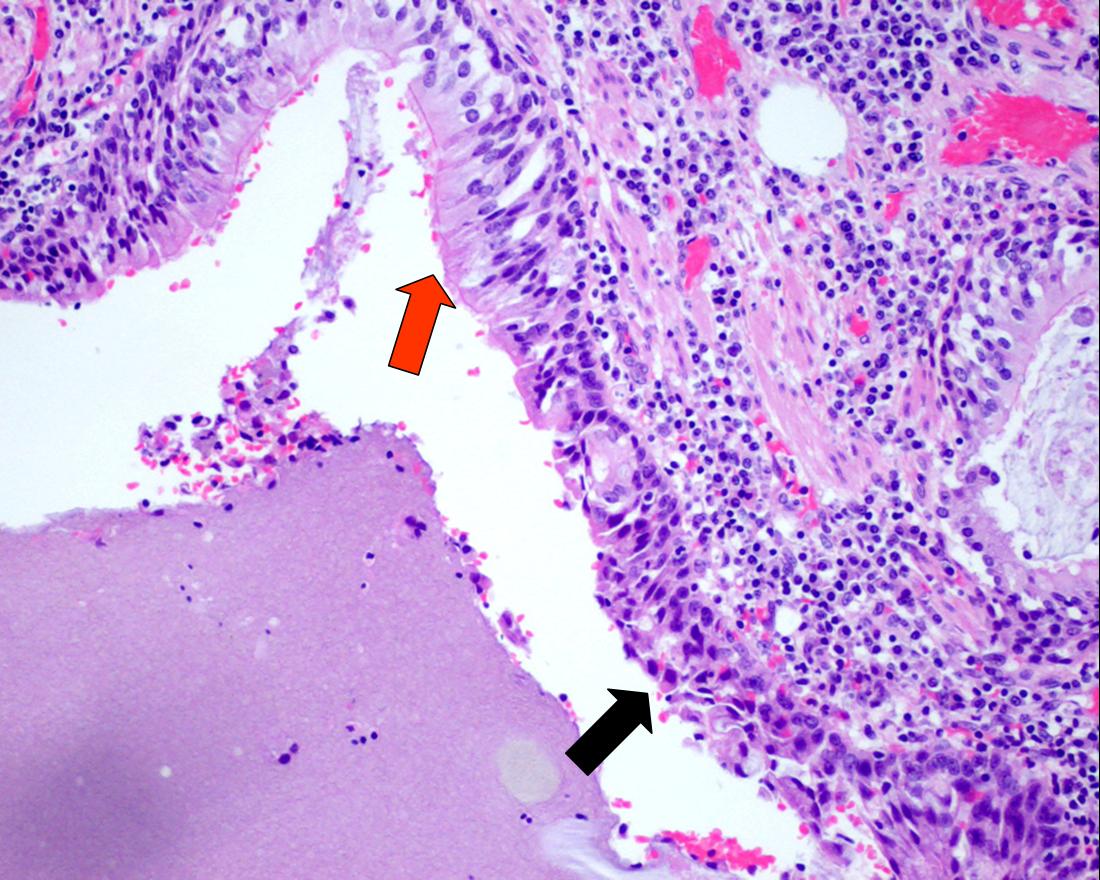
- Respiratory (Ciliated pseudo-stratified columnar epithelium) and GI (squamous epithelium) with reactive changes were found in the same area of fistula. This lumen is not associated with surrounding cartilage. (Figure 8, the red arrow indicates respiratory epithelium, the black arrow indicates GI epithelium)
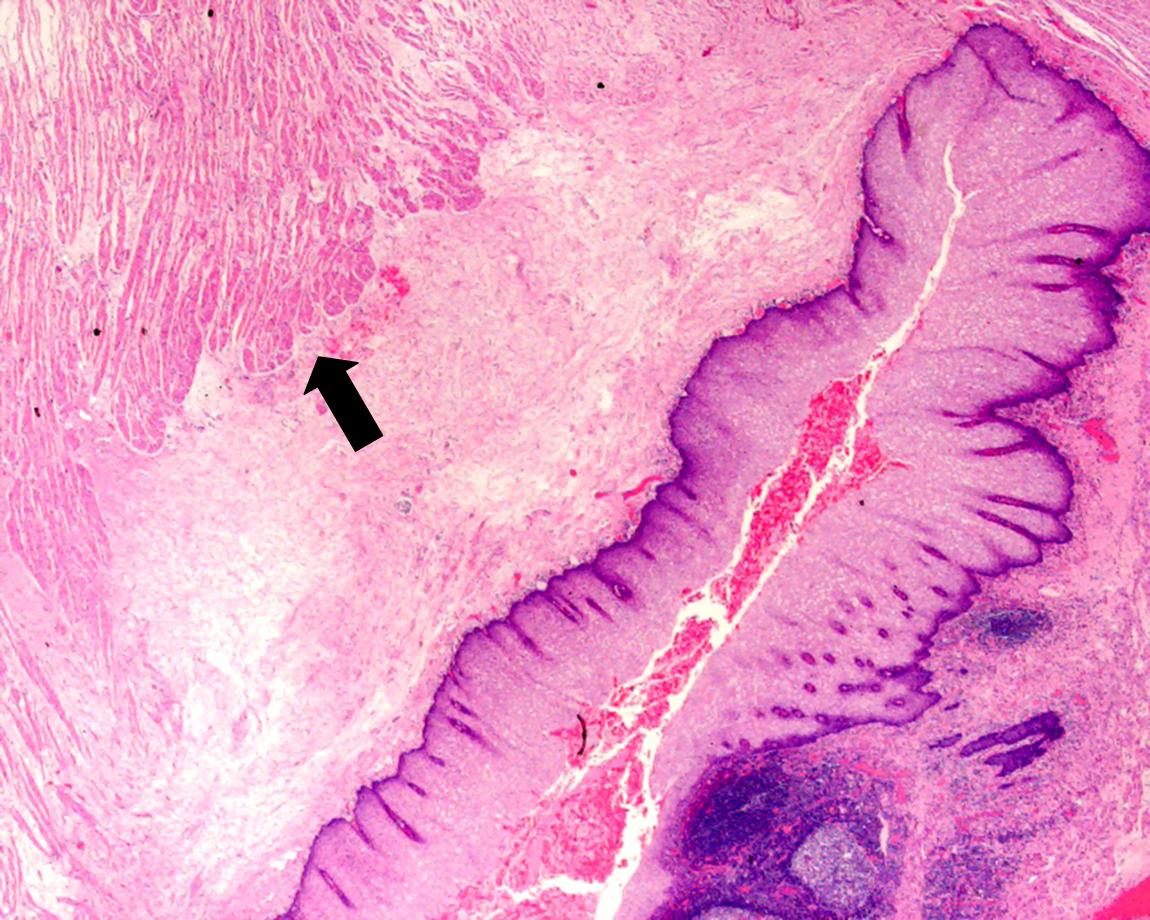
- Presence of normal esophageal structure with two layers of thick smooth muscle with inner circular and outer longitudinal configuration. (Figure 9)
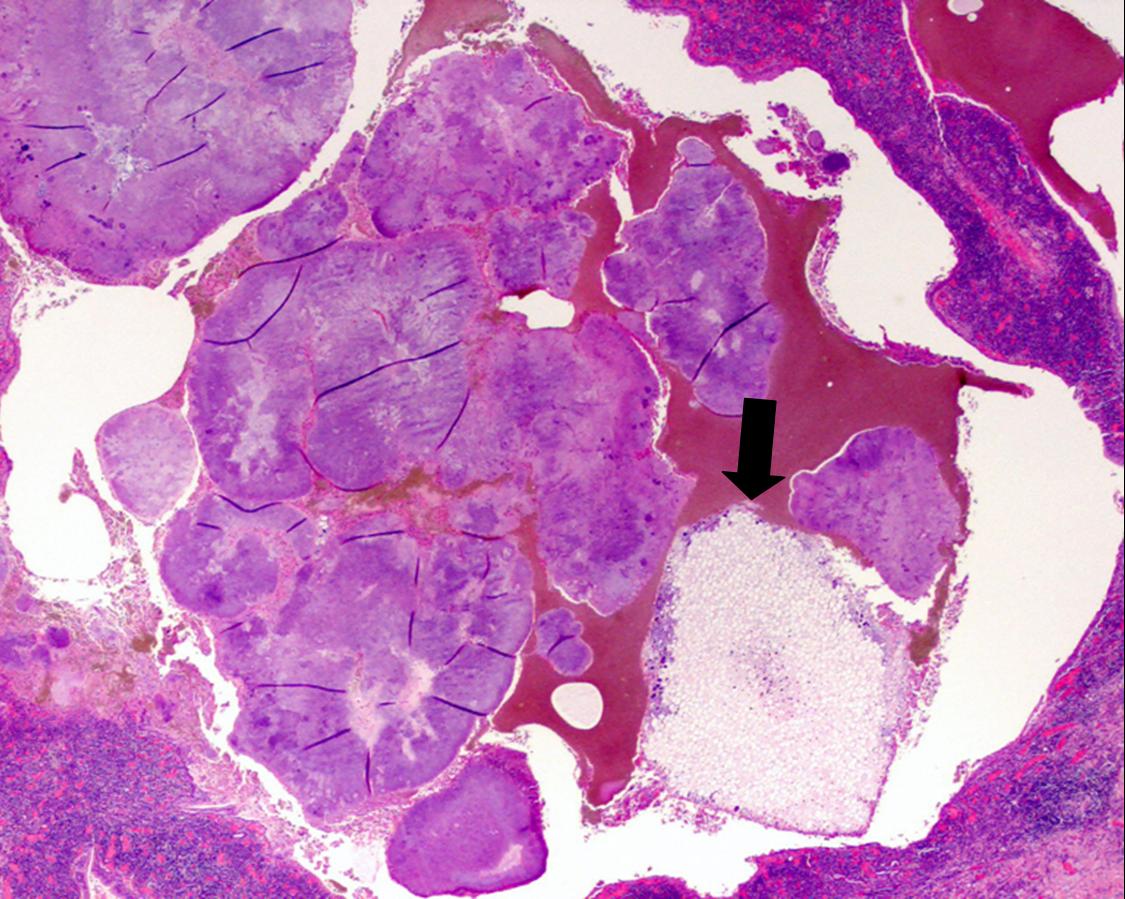
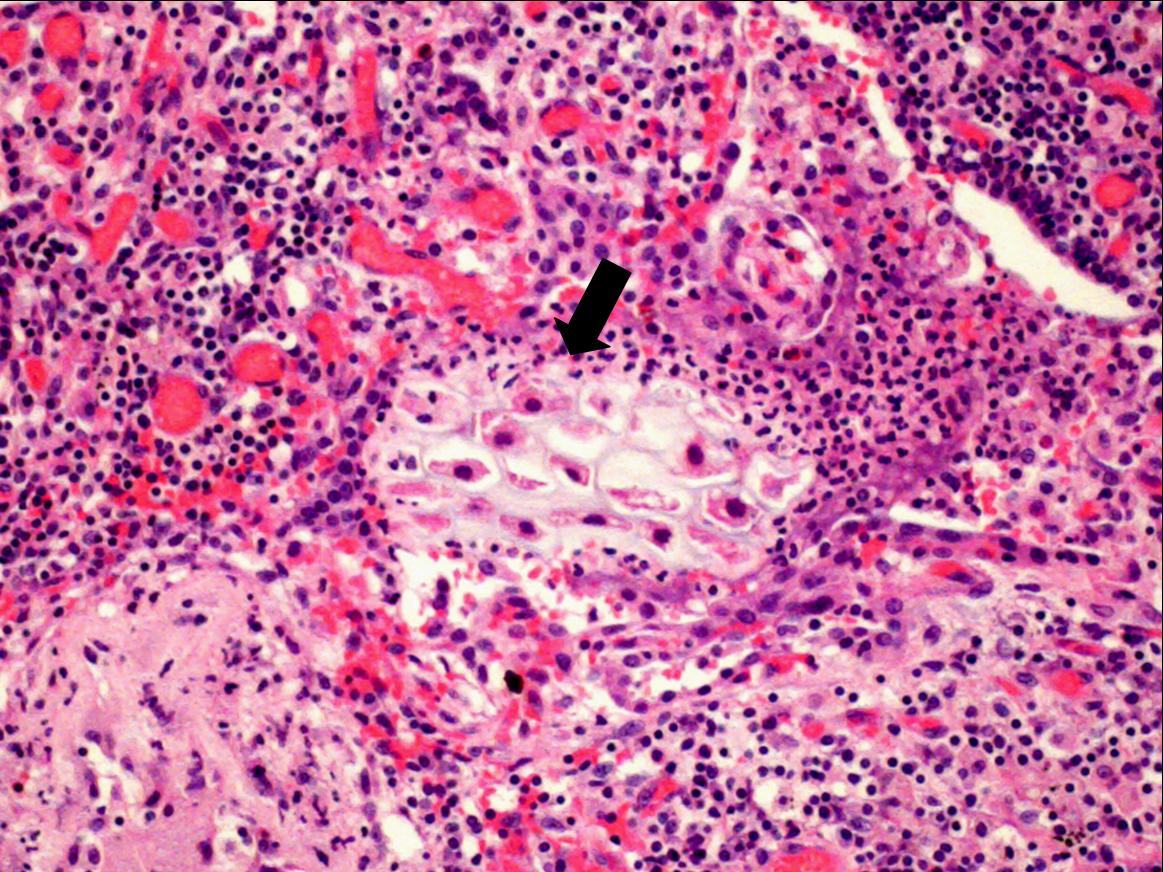
- Food particles, indicated by cell walls of plants with a bacterial colony were found in the airway (bronchioles) (Figure 10-a) and lung parenchyma.(Figure 10-b)
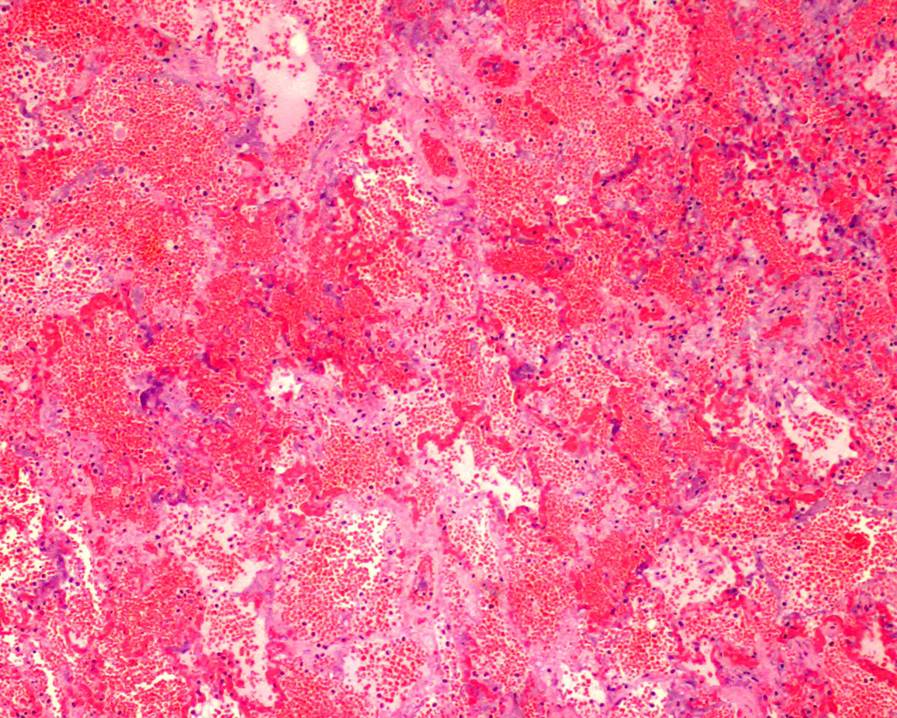
- Diffused alveolar hemorrhage was presented. (Figure 11)
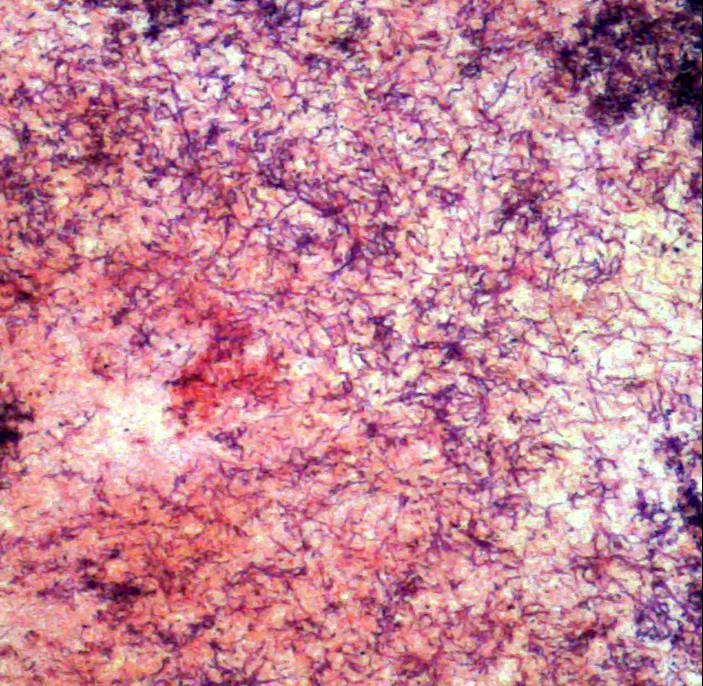
- Gram positive, non-AFB, filamentous agents, consistent with Actinomycetes was noted. (Figure 12-a: Gram stain, Figure 12-b: Gomeri Methanamine stain)
- There were no granulomas, Goblet cell hyperplasia, nor picture of asthma identified from this lung specimen.
The following screen shows pathology images
|

|
| Figure 7-a |
Figure 7-b |
|
| Figure 8 |
|
| Figure 9 |
|
|
| Figure 10-a |
Figure 10-b |
|
| Figure 11 |
|

|
| Figure 12-a |
Figure 12-b |
What is your conclusion and how to explain hemoptysis in this case ?
 Next page
Next page /
