
Page 14 / April 07
Congenital bronchoesophageal fistula is rare. It was first described by Gibson in 1696 and Negusin in 1929. The most recognized classification presented by
Braimbridge and Keith1 in 1965 divide into 4 types as the followings;
Distinguishing congenital from acquired bronchoesophageal fistula is based on the histologic examination. The presence of squamous or columnar epithelium with mucosa and muscularis mucosa suggests a congenital origin; Their absence or presence of inflammatory reaction suggests that fistula was acquired 2,3,9.
The most common chief complaint are postprandial cough (30%) and hemoptysis (23%)5. Esophagography is the most useful diagnostic investigation. Most of cases the fistula was easily visible from esophagoscopy compared to bronchoscopy (11/13 v.s. 4/13)5
The largest review of the Communicating Bronchopulmonary Foregut Malformations (CBPFMs) appeared in 1992 and included 57 patients in a 30-year experience(1959 to 1989)10. Srikanth MS et al proposed the CBPFMs classification be supported by embryogenesis theory.
2. Acquired Bronchoesophageal fistula
There are approximately 40 cases in literature11-14. The most common cause is pulmonary tuberculosis, presenting with mediastinal adenopathy. The histology reveals granuloma and positive Acid Fast Bacilli. The treatment of choice is anti-tuberculous drugs and may proceed to surgical resection if failed medical treatment.
There is a case report of tracheobroncheal foreign body that can cause bronchoesophageal fistula15. However, this is a very rare condition.
 References & Acknowledgements /
References & Acknowledgements /
Discussion - Bronchoesophageal fistula
1. Congenita4l Bronchoesophageal FistulaCongenital bronchoesophageal fistula is rare. It was first described by Gibson in 1696 and Negusin in 1929. The most recognized classification presented by
Braimbridge and Keith1 in 1965 divide into 4 types as the followings;
- type I, with esophageal diverticulum
- type II, direct, short tract from the esophagus to the bronchus
- type III, connect to a cyst in the lobe
- type IV, connect to a sequestrated lung
Distinguishing congenital from acquired bronchoesophageal fistula is based on the histologic examination. The presence of squamous or columnar epithelium with mucosa and muscularis mucosa suggests a congenital origin; Their absence or presence of inflammatory reaction suggests that fistula was acquired 2,3,9.
The most common chief complaint are postprandial cough (30%) and hemoptysis (23%)5. Esophagography is the most useful diagnostic investigation. Most of cases the fistula was easily visible from esophagoscopy compared to bronchoscopy (11/13 v.s. 4/13)5
The largest review of the Communicating Bronchopulmonary Foregut Malformations (CBPFMs) appeared in 1992 and included 57 patients in a 30-year experience(1959 to 1989)10. Srikanth MS et al proposed the CBPFMs classification be supported by embryogenesis theory.
| Group I (16%): | associated with esophageal atresia and tracheoesophageal fistula. |
||
| Group II (33%): | one lung originates from the lower esophagus. |
||
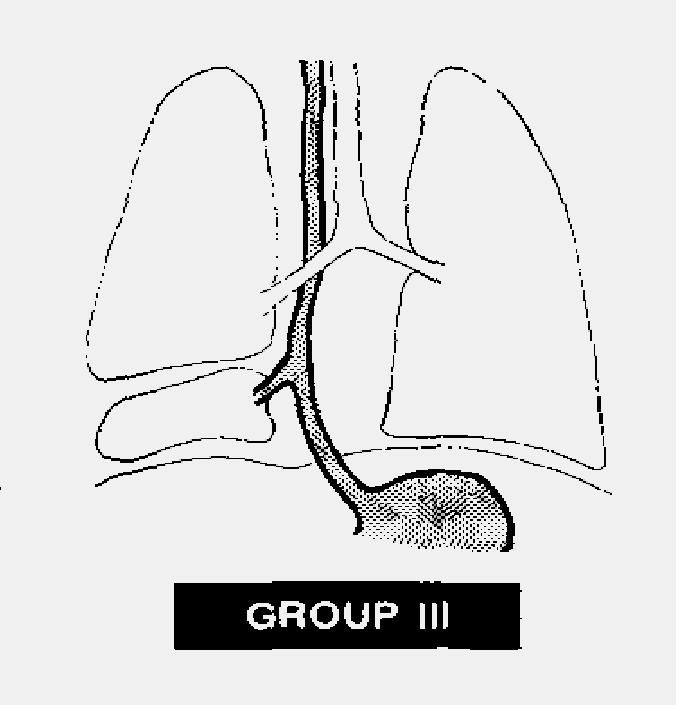
| Group III (46%): | isolated anatomic lung lobe or segment (extralobar sequestration) communicates with the esophagus or stomach (Figure 13)
|
||
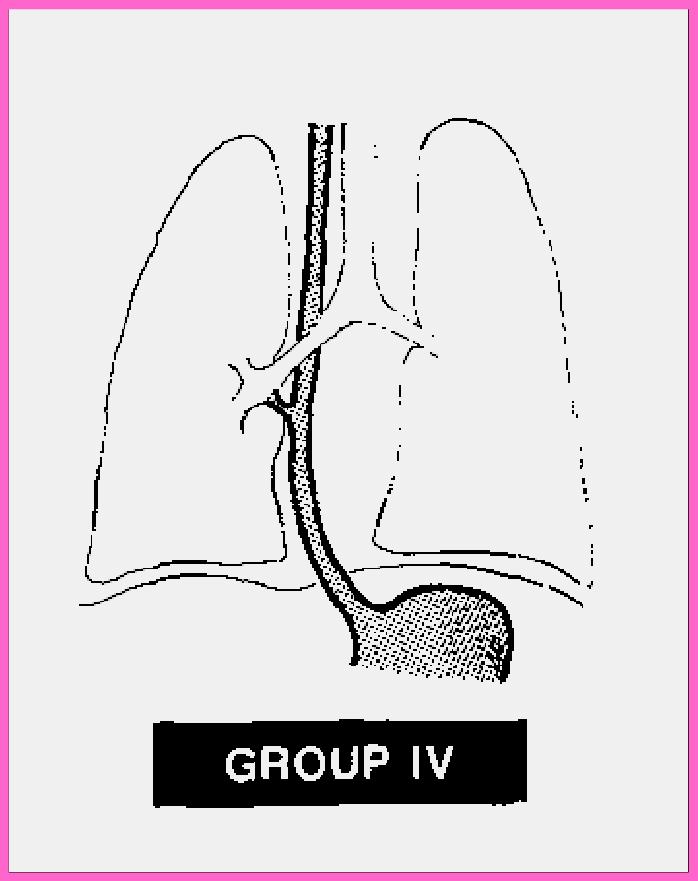
| Group IV (5%): | portion of the normal bronchial system, mostly from right lung, communicates with the lower esophagus, similar to our patient. (Figure 14)
|
2. Acquired Bronchoesophageal fistula
There are approximately 40 cases in literature11-14. The most common cause is pulmonary tuberculosis, presenting with mediastinal adenopathy. The histology reveals granuloma and positive Acid Fast Bacilli. The treatment of choice is anti-tuberculous drugs and may proceed to surgical resection if failed medical treatment.
There is a case report of tracheobroncheal foreign body that can cause bronchoesophageal fistula15. However, this is a very rare condition.