
Page 8 / January 07
- Chylothorax: is the occurrence of chyle (lymph) in the pleural cavity.
- Chyle: is lymphatic fluid enriched with fat secreted by intestinal cells.
Features of chyle include the following: triglyceride concentration of more than 1.1mmol/L "100mg/dL", lipid electrophoresis showing chylomicrons, absolute cell count of more than 1000 cells/µL with lymphocyte fraction of more than 60-90%. Less than 50% of chyle appeared milky. Average chyle output in adults around 1.5-2.5 L/Day. It has a bacteriostatic property and almost always sterile. Protein and other chemical component usually similar to those of serum with PH = 7.4.
- Pseudochylothorax (cholesterol pleurisy):
Occurs with long-standing fluid in a fibrotic pleura, characterized by a very high content of cholesterol. Triglyceride content is not specific but characteristically lipid electrophoresis shows no chylomicrons.
Both chylothorax and pseudochylothorax have a common characteristic: the pleural fluid is usually thick, opalescent, whitish or the color of café-au-lait or chocolate milk, due to its very high fat content. Apart from that, they have nothing in common.
Anatomy and Physiology:
The lymph vessels from the peritoneal cavity and the lower parts of the body come together behind the aorta, below the diaphragm, and form the thoracic duct. Usually, there is a widening of the duct at its origin, which has been termed the cisterna chyli. The duct passes through the diaphragm behind the aorta, and runs upwards on the right side of the vertebral column between the azygos vein and the aorta. At the level of the third or fourth vertebra, it turns to the left, crosses the mid-line, and continues upwards behind the oesophagus, medially of and behind the subclavian artery. It then turns laterally, often after making a small loop up into the neck region, and finally empties into the vena subclavia between the jugular and the vertebral veins.
This anatomy explains why a chylothorax is usually right-sided, since the largest part of the duct is within the right hemithorax. It has to be realized, however, that the anatomy of the duct can vary considerably. Tow or more branches of the duct can be seen, and the duct can even empty into the right subclavian vein.
The thoracic duct contains many valves forcing the chylus in one direction only. Movement of the thorax propels the chyle forwards. There are numerous small connections with veins, making it possible to ligate the ductus without any resulting problems.
Apart from its protein and fat content, the chyle also contains a large number of lymphocytes and is bacteriostatic. The normal daily flow of chylus in an adult is around 2L. The flow of chylus increases substantially with intake of food and drink, and decreases to a small trickle with starvation. With repeated thoracocenteses or continuous drainage of a chylothorax, large amount of fat, proteins and lymphocytes are lost, quickly resulting in negative effects on the patient's nutritional and immunological status.
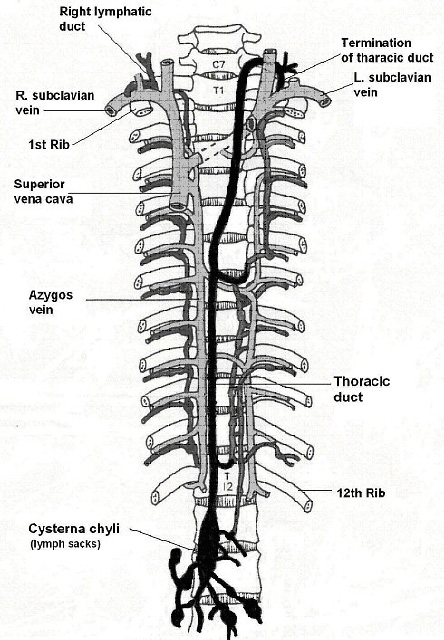
Figure 3
Aetiology of chylothorax:
Chylothorax is due to leakage of chyle from the thoracic duct. This in turn is due to a variety of causes, for simplification these can be divided to traumatic or non-traumatic.
"see the table below". Thoracic duct is a fairly weak, and in fact, and even an intense sudden stretching of it can cause rupture, as has been described after forceful cough, emesis, or the strains of childbirth, more usually in the infant but also encountered in the mother.
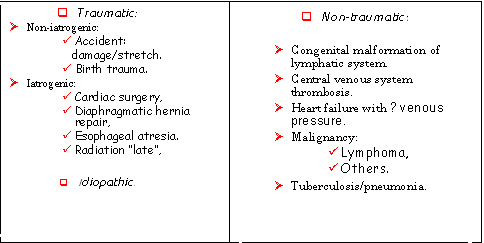
Table 1.
Among the traumatic causes post-surgical chylothorax accounts for 65-85% in pediatric population, with the cardiac surgeries as the major contributor, with an incidence of 0.25-5.3%. Chylothorax usually appears 1-21 days post-surgery.
For non-traumatic causes, congenital malformation of lymphatic system has been estimated to account for 8%, while significant increase in central venous system pressure, secondary to congestive heart failure or thrombosis of superior vena cava or other central vein, accounts for 27% of total childhood chylothorax.
Congenital chylothorax has been reported in association with single umbilical artery and chromosomal abnormalities namely trisomy 21, trisomy 10 and Turner syndrome. Defects could include complete atresia of the thoracic duct, lymphangiomatosis or lymphangiectasia. Complication of congenital chylothorax includes pulmonary hypoplasia and fetal hydrops.
Treatment:
The standard treatment of chylothorax in children includes conservative therapy, with dietary strategy or pharmacological agents, as a first line of management and, if this is not successful, surgical interventions would be the ultimate choice.
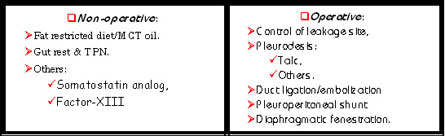
Table 2.
Dietary strategy includes fat restricted diet and use of median chain triglyceride (MCT) oil, aiming for reduction in chyle production. Effect starts to manifest 3-5 days from starting those measures, with a success rate of 50-80%. Albumen, immunoglobulins, fibrinogen, prothrombin and electrolytes should be monitored because of high demand related to chyle loss. (See appendix for sample of fat restricted dietary list and formulas from: Management of chylothorax in children by: E. C. Suddaby and S. Schiller ).
If 1-2 weeks of restricted dietary management fails to decrease chyle production, gut rest and total parenteral nutrition (TPN) should be initiated, again aiming to reduce chyle production, as some studies showed that only sterile water ingestion can stimulate chyle flow by 20%.
Pharmacological treatment includes somatostatin analog, which has been used for the first time in 1990 for management of chylothorax in adults, and then in 2003 in neonates. Octreotide is a synthetic analog of somatostatin, can be administered either intravenously or subcutaneously, in a dose of 1-4 µg/kg/hr. The mechanism of action that has been proposed is via a vasoconstriction of splanchnic vessels leading to reduction in gastric, pancreatic, and intestinal secretion, as well reduction in intestinal absorption and hepatic venous flow. Side effects are rare and include: hypoglycemia, hypothyroidism and liver toxicity. One case report questioned necrotizing enterocolitis (NEC) as a possible complication in a neonate who developed chylothorax post aortic coarctation repair which could cause NEC by bowel ischemia. Other side effects include: vomiting and risk of arrhythmias including bradycardia, conduction abnormalities such as heart blocks, and prolongation of the QT interval. Because many patients with chylothorax have cardiac problems, they should be monitored for these possible side effects.
The substitution of factor XIII with an application of recombinant factor XIII rapidly reduces the amount of chylous effusion after pediatric open heart surgery.
Surgical management of chylothorax is usually considered as the last resource of treatment if conservative therapy failed to control chyle leakage. This includes: control of leakage site if identified, thoracic duct ligation or embolization, pleuroperitoneal shunt and diaphragmatic fenestration. Pleurodesis with talc or other sterile irritant agent reported in some resistant cases to control chylothorax by obliterating pleural cavity secondary to fibrous adhesion.
Specific antenatal therapeutic measures for congenital chylothorax include: maternal dietary modification, repeat thoracocentesis, thoracoamniotic shunting, intrapleural injection of maternal blood and pleurodesis with OK-432.
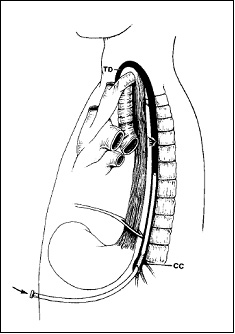
Figure 4.
Transcutaneous embolization of thoracic duct
From: Treatment of chylothorax by lymphatic embolization and disruption, By: C. Cope & L. R. Kaiser 2002 JVIR
 References /
References /
"Chylothorax in children"
Definition:- Chylothorax: is the occurrence of chyle (lymph) in the pleural cavity.
- Chyle: is lymphatic fluid enriched with fat secreted by intestinal cells.
Features of chyle include the following: triglyceride concentration of more than 1.1mmol/L "100mg/dL", lipid electrophoresis showing chylomicrons, absolute cell count of more than 1000 cells/µL with lymphocyte fraction of more than 60-90%. Less than 50% of chyle appeared milky. Average chyle output in adults around 1.5-2.5 L/Day. It has a bacteriostatic property and almost always sterile. Protein and other chemical component usually similar to those of serum with PH = 7.4.
- Pseudochylothorax (cholesterol pleurisy):
Occurs with long-standing fluid in a fibrotic pleura, characterized by a very high content of cholesterol. Triglyceride content is not specific but characteristically lipid electrophoresis shows no chylomicrons.
Both chylothorax and pseudochylothorax have a common characteristic: the pleural fluid is usually thick, opalescent, whitish or the color of café-au-lait or chocolate milk, due to its very high fat content. Apart from that, they have nothing in common.
Anatomy and Physiology:
The lymph vessels from the peritoneal cavity and the lower parts of the body come together behind the aorta, below the diaphragm, and form the thoracic duct. Usually, there is a widening of the duct at its origin, which has been termed the cisterna chyli. The duct passes through the diaphragm behind the aorta, and runs upwards on the right side of the vertebral column between the azygos vein and the aorta. At the level of the third or fourth vertebra, it turns to the left, crosses the mid-line, and continues upwards behind the oesophagus, medially of and behind the subclavian artery. It then turns laterally, often after making a small loop up into the neck region, and finally empties into the vena subclavia between the jugular and the vertebral veins.
This anatomy explains why a chylothorax is usually right-sided, since the largest part of the duct is within the right hemithorax. It has to be realized, however, that the anatomy of the duct can vary considerably. Tow or more branches of the duct can be seen, and the duct can even empty into the right subclavian vein.
The thoracic duct contains many valves forcing the chylus in one direction only. Movement of the thorax propels the chyle forwards. There are numerous small connections with veins, making it possible to ligate the ductus without any resulting problems.
Apart from its protein and fat content, the chyle also contains a large number of lymphocytes and is bacteriostatic. The normal daily flow of chylus in an adult is around 2L. The flow of chylus increases substantially with intake of food and drink, and decreases to a small trickle with starvation. With repeated thoracocenteses or continuous drainage of a chylothorax, large amount of fat, proteins and lymphocytes are lost, quickly resulting in negative effects on the patient's nutritional and immunological status.
Figure 3
Aetiology of chylothorax:
Chylothorax is due to leakage of chyle from the thoracic duct. This in turn is due to a variety of causes, for simplification these can be divided to traumatic or non-traumatic.
"see the table below". Thoracic duct is a fairly weak, and in fact, and even an intense sudden stretching of it can cause rupture, as has been described after forceful cough, emesis, or the strains of childbirth, more usually in the infant but also encountered in the mother.
Table 1.
Among the traumatic causes post-surgical chylothorax accounts for 65-85% in pediatric population, with the cardiac surgeries as the major contributor, with an incidence of 0.25-5.3%. Chylothorax usually appears 1-21 days post-surgery.
For non-traumatic causes, congenital malformation of lymphatic system has been estimated to account for 8%, while significant increase in central venous system pressure, secondary to congestive heart failure or thrombosis of superior vena cava or other central vein, accounts for 27% of total childhood chylothorax.
Congenital chylothorax has been reported in association with single umbilical artery and chromosomal abnormalities namely trisomy 21, trisomy 10 and Turner syndrome. Defects could include complete atresia of the thoracic duct, lymphangiomatosis or lymphangiectasia. Complication of congenital chylothorax includes pulmonary hypoplasia and fetal hydrops.
Treatment:
The standard treatment of chylothorax in children includes conservative therapy, with dietary strategy or pharmacological agents, as a first line of management and, if this is not successful, surgical interventions would be the ultimate choice.
Table 2.
Dietary strategy includes fat restricted diet and use of median chain triglyceride (MCT) oil, aiming for reduction in chyle production. Effect starts to manifest 3-5 days from starting those measures, with a success rate of 50-80%. Albumen, immunoglobulins, fibrinogen, prothrombin and electrolytes should be monitored because of high demand related to chyle loss. (See appendix for sample of fat restricted dietary list and formulas from: Management of chylothorax in children by: E. C. Suddaby and S. Schiller ).
If 1-2 weeks of restricted dietary management fails to decrease chyle production, gut rest and total parenteral nutrition (TPN) should be initiated, again aiming to reduce chyle production, as some studies showed that only sterile water ingestion can stimulate chyle flow by 20%.
Pharmacological treatment includes somatostatin analog, which has been used for the first time in 1990 for management of chylothorax in adults, and then in 2003 in neonates. Octreotide is a synthetic analog of somatostatin, can be administered either intravenously or subcutaneously, in a dose of 1-4 µg/kg/hr. The mechanism of action that has been proposed is via a vasoconstriction of splanchnic vessels leading to reduction in gastric, pancreatic, and intestinal secretion, as well reduction in intestinal absorption and hepatic venous flow. Side effects are rare and include: hypoglycemia, hypothyroidism and liver toxicity. One case report questioned necrotizing enterocolitis (NEC) as a possible complication in a neonate who developed chylothorax post aortic coarctation repair which could cause NEC by bowel ischemia. Other side effects include: vomiting and risk of arrhythmias including bradycardia, conduction abnormalities such as heart blocks, and prolongation of the QT interval. Because many patients with chylothorax have cardiac problems, they should be monitored for these possible side effects.
The substitution of factor XIII with an application of recombinant factor XIII rapidly reduces the amount of chylous effusion after pediatric open heart surgery.
Surgical management of chylothorax is usually considered as the last resource of treatment if conservative therapy failed to control chyle leakage. This includes: control of leakage site if identified, thoracic duct ligation or embolization, pleuroperitoneal shunt and diaphragmatic fenestration. Pleurodesis with talc or other sterile irritant agent reported in some resistant cases to control chylothorax by obliterating pleural cavity secondary to fibrous adhesion.
Specific antenatal therapeutic measures for congenital chylothorax include: maternal dietary modification, repeat thoracocentesis, thoracoamniotic shunting, intrapleural injection of maternal blood and pleurodesis with OK-432.
Figure 4.
Transcutaneous embolization of thoracic duct
From: Treatment of chylothorax by lymphatic embolization and disruption, By: C. Cope & L. R. Kaiser 2002 JVIR
Sample of fat restricted formulas
Sample of fat restricted dietary list
Pennington, J.A.T. (1994) Bowes & Church's
food values of portions commonly
used (16th edition). Philadelphia, PA:
J.B. Lippincott Company.
Sample of fat restricted dietary list
Pennington, J.A.T. (1994) Bowes & Church's
food values of portions commonly
used (16th edition). Philadelphia, PA:
J.B. Lippincott Company.