
PULMONARY
ALVEOLAR PROTEINOSIS
Pulmonary alveolar proteinosis is a rare disease and this case shows
some clinical issues that pulmonologists face in dealing with this disease.
It is important for pulmonologists to know about this disease and treatment
options and considerations. I will now review the literature on pulmonary
alveolar proteinosis.
The
following sections will cover:
–
Definition
–
Surfactant
Review
–
Types
of alveolar proteinosis: congenital
alveolar proteinosis (SP-B deficiency) acquired alveolar proteinosis
–
Historical
–
Epidemiology
–
Pathogenesis
–
Clinical
Manifestations
–
Diagnosis
–
Treatment
–
Prognosis
–
Application
to this case
Pulmonary
Alveolar Proteinosis
–
Non-inflammatory
lung disease
–
Syndrome
characterized by alveolar filling with surfactant-associated lipids
and proteins
–
No
structural airway abnormalities and no fibrosis
Pulmonary
Surfactant Review
–
Composition
of surfactant in humans: 90% phospholipid, 10% protein, minimal carbohydrate
–
Premature
infants are deficient in phosphotidylcholine, phosphotidylglycerol
–
Exogenous
surfactant restores function by reconstituting phospholipids
–
Four
surfactant proteins: (A, B, C, D) have been characterized at a moelcular
level.
BELOW: Biosynthesis of surfactant protein B. CLICK FOR AN ENLARGEMENT.
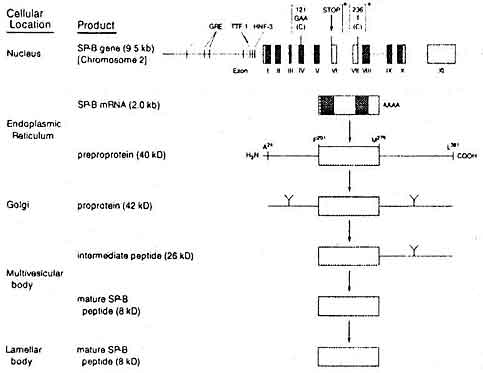
Phospholipid components of surfactant are synthesized from choline and fatty acid precursors in the endoplasmic reticulum and Golgi apparatus of type II alveolar cells. The SP-B gene on chromosome encodes mRNA, which in turn directs the translation of a preprotein. The protein is then processed from a multivesicular body to give rise to a lamellar body. The lamellar bodies and then extruded into the alveolar lumen where they form tubular myelin. This makes up the underlying latticeowrk upon which the phospholipid film lies. The film and the latticework are then degraded and cycled back by the type II pneumocytes or the taken up by alveolar macrophages.
Cellular
and Molecular of Surfactant Protein-B (SP-B)
–
SP-B
exclusively found in human lungs, in type II pnuemocytes
–
Function
- increases organization of phospholipid film, which is required to
decrease surface tension in alveoli: SP-B is necessary for formation
of tubular myelin
–
Regulation
- there are glucocorticoid response elements in the promoter region
which facilitate surfactant synthesis.
–
Activity
- an anti-SP-B antibody had been identified and plays a role in pulmonary
inflammation
SP-B
Deficiency In Humans
–
First
described in family of 3 infants (Nogee, 1993, NEJM, )
–
Respiratory
failure at birth despite being term infants - congenital alveolar proteinosis
–
Mode of transmission is autosomal recessive, lethal disease without
transplantation
–
30
subsequent families, 50 infants have been identified (1997)
–
Rare,
probably underrecognized
a)
Molecular Aspects
–
2
mutations: which result in unstable transcription:
121ins2 mutation - Substitution of three bases for single nucleotide
Premature termination signal as a result of a frameshift mutation
Most common, accounts for 75% of alleles in SP-B deficient patients
R236C muatation - Nucleotide substitution which resulted in alteration of the amino acid
– Heterogenous disease - ? phenotypic variations
b)
Clinical Features of SP-B Deficiency
–
Born
at or near term, clinically and radiographically similar to hyaline
membrane disease with severe, progressive respiratory failure.
–
There
may be a family history:
–
Homozygotes:
Aggressive supportive interventions do not help including: surfactant
replacement, corticosteroids, ECMO
–
Heterozygotes:
low, but detectable SP-B in tracheal fluid may benefit from steroids,
spontaneous resolution has been reported
–
5
survivors total in literature despite onset in infancy which may represent
a heterogenous disease.
–
Adding
SP-B did not help, death at age 54 days (Hamvas, 1994, J Peds)
c)
Biochemical Features of SP-B Deficiency
–
Complete
lack of immunoreactive SP-B
–
Abnormal
surfactant composition and function: increased accumulation of proSP-C
and an aberrant form of SP-C
–
Role
in pathophysiology of SP-B not yet known
d)
Treatment and Prognosis of SP-B Deficiency
–
Rapid
fatal outcome without prompt recognition and treatment.
–
Lung
transplant; only available option, but longest reported survival was
34 months as of 1996 (Hamvas, 1997, Adv in Peds)
–
Other
temporizing measures: glucocorticoids, SP-B replacement have been tried,
BAL - no long term benefit
–
? potential role for gene therapy in the future