
Carcinoid tumors are also associated with other malignancies; specifically in the form of multiple neuroendocrine neoplasia syndromes (MEN). A study by Duh et al. suggested that 4% of all carcinoid tumors have endocrinologic malignancies.2 When associated with MEN, 47% of bronchial carcinoid patients had a pituitary tumor. It is important to keep this in mind when treating a patient with bronchial carcinoid.
Carcinoid tumors can also cause a variety of systemic symptoms by production of different hormones. ACTH, gastrin, insulin, vasoactive intestinal peptide, serotonin and histamine have all been reported.16 A review by Amer et al. found that 4% of pulmonary carcinoids were associated with Cushing's syndrome.17 These patients presented with hypertension, cushingoid habitus, muscle weakness and a hypokalemic alkalosis. Carcinoid syndrome is caused by serotinin release from the tumor. 10 to 30% of patients with carcinoid tumors may have this syndrome.18 It is more frequent with larger tumors, tumors that drain into the systemic circulation and those that have metastasized especially with liver involvement.19 Carcinoid syndrome can produce a variety of symptoms including flushing of the skin, diarrhea and endocardial fibrosis.20,18 Wheezing can occur in 20% of patients. Diagnosis can sometimes be delayed because of the confusing array of symptoms at presentation.
In summary, bronchial carcinoid tumors are rare in both children and adults. Presentation can be varied which can delay the diagnosis. Treatment is surgical and survival is generally good but one must be vigilant for recurrences and associated tumors.
CASE CONSLUSION
After the biopsy results were known, the history was again reviewed to look for signs or symptoms of para-neoplastic syndromes or metastases. There was no new information gained however, he did complain of headaches and abdominal pain intermittently. A CT scan of his head and abdomen were arranged. Both were interpreted as normal. An octreotide scan showed uptake only in the area of the tumor. After discussion regarding the best course of surgical management he underwent a completion pneumonectomy and node dissection. One node was positive.
He is currently doing well post surgery. He continues to have a mild cough but has had no further admissions. A follow-up octreotide scan 6 months post surgery showed no evidence of recurrence or metastases. (See attached scans.) He will be undergoing a complete endocrine evaluation in the near future.
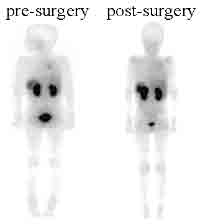
ENLARGE the follow-up octreotide scan.
IN RETROSPECT
In retrospect, his first chest x-ray did show inversion of his right hemi-diaphragm which may have raised the possibility of an obstructive lesion causing hyperinflation; especially with a past history of a presumed foreign body.
In addition, his pulmonary function tests suggested hyperinflation in the presence of a non-reversible obstructive defect. His peak flows, in addition to his mid expiratory flows, were low and did not reverse with bronchodilator. These observations would not be consistent with asthma but fit with a diagnosis of a 'ball valve' obstruction of a large airway. His second chest x-ray with volume loss on the right side would be consistent with complete obstruction of the bronchus.